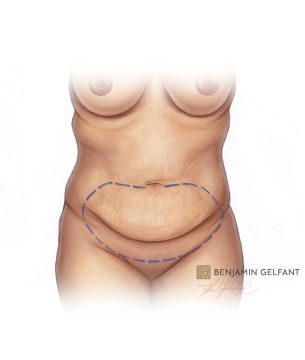
A tummy tuck (also known as abdominoplasty) is a cosmetic procedure that flattens the abdomen by removing excess fat and skin while tightening muscles in abdominal wall.
No matter how hard you exercise, and no matter how diligent you are with your diet, sometimes (especially after pregnancy has separated the muscles), the only remedy is a tummy tuck.
Next to concern with breast size, shape and position the most common request for help we see is with the abdomen and the body “core”.
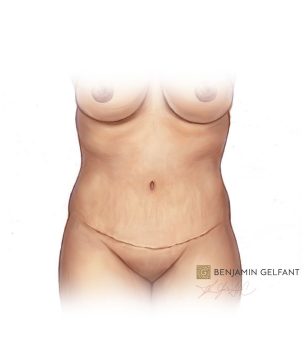
I aim to get you confident enough in your appearance for you to get back into a two piece bathing suit, and while we can’t guarantee this will occur, in most cases it does. Think how much better you would feel if you no longer felt like covering up.

Special Featured Video
Abdominoplasty (Tummy Tuck) with Liposuction
Video shows actual footage of the operation, some viewers may find scenes disturbing.
**Viewer discretion advised
Watch Video Now
Introduction to Abdominoplasty / Tummy Tuck
The most common body contouring operation, aside from liposuction, is abdominoplasty, or the tummy tuck. This involves three or four elements:
- Removal of excess skin
- Tightening the abdominal muscles
- Relocating the belly button (umbilicus)
- (commonly) removal of fat in the upper abdomen and sides (flanks)
Looking For More Procedure Information?
Submit your email and receive Dr. Gelfant's illustrated patient guides in your inbox.
FAQs
Should I wait to have a “tummy tuck”until I have had all my children?
In general, if you are planning to have more children, some of the benefits may be lost. However, if you have lost weight and have excess skin as a result, feel self-conscious about your appearance, the results of surgery may justify the operation at any time.
Won’t liposuction take care of it?
When there is skin looseness and the underlying muscles are stretched, suction will not improve the appearance and may worsen it. When there is significant fat and some skin looseness, suction won’t give a satisfying result, and may even, make matters worse. Once in a while, I see a patient for whom it’s reasonable to start with a preliminary suction operation, with the understanding that a secondary tummy tuck may be needed.
Do I need to have such a long scar?
The incision length depends mostly on how wide an area of skin is removed, and this is related to how loose the skin is. In an abdominoplasty (tummy tuck), when all the skin below the belly button is removed, the scar usually runs from hip to hip. Less looseness requires a smaller incision.
When can I start exercising again?
I encourage walking during the first few days, light aerobic activity at two weeks, and full exercise routine with abdominal exercises at six weeks.
What about Cool®Sculpting and other non-surgical treatments?
Again, if you have loose skin and muscles, this won’t help.
Patient Resources
Abdominoplasty Surgery Instructions
Download PDFAdditional Info.
Incision
Although mini-tummy tucks, which involved smaller incisions, were popular when I first started practice, the results often were significantly compromised and a return to longer incisions became the usual approach. As with small incision breast lifts, scars fade over time, but if the contours aren’t improved dramatically, a shorter scar is no advantage. The average patient, who comes with skin looseness (“laxity”) and some excess abdominal fat after pregnancies or previous surgery needs a full abdominoplasty with a traditional incision. In fact, the most common form of abdominoplasty which I currently use is not a lesser variation of a traditional procedure, but is, instead, more extensive, because so much more is known about how to achieve the best results.
The incision is planned carefully, taking into account the bathing suit and undergarment lines. I go over this at the time of consultation with patients and suggest we mark the incision with her standing and wearing undergarments prior to surgery.
Anaesthesia
Surgery is done under general anesthesia (completely asleep). We add local anaesthetic by injecting it at the start of and during surgery which helps to minimize post-operative pain.
Procedure
Once you are put to sleep, and the torso has been washed with antiseptics and surrounded with sterile towels, the operating team has done a final “time-out” safety checklist.
If liposuction is going to be done we do it first, through small incisions, usually within the skin area that is going to be removed.
The incision is now created and the skin of the abdomen is separated from the underlying muscle layer, first up to the belly-button, which is next separated from the surrounding skin and left in place, we then carry on into the upper abdomen and up to the bottom of the breastbone, minimizing how much we separate the skin near the rib margins in order to preserve circulation and sensation as much as possible.
The muscles of the abdominal wall are now visible, and the rectus abdominis muscles (the ones you use to do “crunches” and “sit-ups”) nearly always are separated after pregnancy (diastasis recti). I bring the muscles back together with a series of stitches in two layers.
Skin Removal (resection) and repair
Here’s where I get to be a tailor, a disappearing craft, in our culture.
Traditional abdominoplasty involved until the surgeon could bring the cut edge at the top of the belly button hole and removing everything in between, often needing to flex the surgery bed to an extreme, just to bring those edges together, and with no regard to any other judgement. This often left patients unable to stand up straight for weeks and weeks. It also put a lot of strain on the incision repair, and led to all sorts of healing problems and widening of scars. I think it also caused an increased risk of Venous thrombosis (blood clot), a feared and potentially lethal complication.
Tummy tucks no longer rely on skin tension for getting good results. Dr. Ted Lockwood, who practiced in Kansas city, revolutionized body contour surgery with his careful study of anatomy and applied his knowledge of the superficial fascial system (SFS) to put tension on the tissues than can really support the repair and leave little tension on the skin. I was fortunate to hear Dr. Lockwood in my early practice years and, later, see him operate. His techniques struck me profoundly right away, as they resonated with the same ideas which had come earlier in facelift surgery.
As a result, we first estimate the amount of skin removal with gentle flexion of the OR bed, and then proceed to use a series of “basting” stitches in the SFS to further refine that estimate. Finally, the skin removal takes place with minimal tension planned.
Aftercare and Recovery
I keep my tummy tuck patients overnight. Most of my patients have small kids at home and it is impossible to get started on recovery properly when, naturally, they want your attention. But even when that’s not the case, going home immediately after a tummy tuck is not easy, no matter what pain relievers are used or whether there is a local anaesthetic “pain pump” (I don’t use them) used. Spending a night in clinic is never seen as a waste. You are in expert hands with professional experienced nurses and I think this enhances the recovery. Intermittent venous compression pumps are used to keep blood flow in the legs until patient is up and moving about. The nurses give post-op teaching especially about our preventive measures for venous thrombosis and I see my patient the morning after surgery.
The drains come out at somewhere between six and eight days after surgery, on average. In the first week, walking about is a little uncomfortable and this changes quickly after drains are removed so they can stand up straight.
Most patients are back to work in two weeks. We begin exercise with walking early, and progress rapidly during the time from two to six weeks. Abdominal exercise can be started as early as a month in selected cases and almost always by six weeks.
Scars heal (mature) according to a schedule individual to each person, but generally look their worst between 6 and 8 weeks after surgery, stabilize, and then begin to soften and fade, a process that takes from six to twenty-four months.
Risks
- Infection
- Bleeding
- Seroma
- Venous thrombosis and pulmonary embolus
- Wound healing complications (necrosis etc)
Abdominoplasty, and the related body contouring operations, all share similar risks and possible complications. Like all surgical procedures, bleeding or infection can occur, although both are unusual. If they do occur, they may require surgical treatment, hospitalization, or may be managed with lesser measures in some cases. Infection, when diagnosed early and not severe, may respond to antibiotics by mouth, for example.
Seroma is discussed above under the use of drains.
Problems with poor or delayed healing of the incision can occur, leaving areas with widened scars after crust formation. This is a many times greater risk in smokers. All smokers must quit for this surgery.
Blood clots can form in the legs (thrombophlebitis), with possible passage of a clot to the lungs. While rare, this is potentially a lethal problem. At one time, abdominoplasty patients were routinely kept on bed rest for several days after surgery; today, patients are routinely up and walking within a day or so after surgery. Early mobilization has always been felt to be one of the best preventive measures against thrombophlebitis, and we believe it to be of value in body contour surgery. However, several years ago I attended a safety course at the American Society for Aesthetic Plastic Surgery (ASAPS) annual meeting. There was strong evidence in favour of putting all tummy tuck patients on post-op blood thinners and I have done so ever since. I have been fortunate in that I have never had a patient develop an embolus or even clinically evident venous thrombosis. BUT our routine is:
- ALL patients must stop birth control pills and hormone replacement therapy
- All smokers must quit
- All cases have pneumatic compression devices on their legs during and after surgery
- All major body contour surgery patients are treated preventively with blood thinners (fractionated heparin)
- We encourage early mobilization and ambulation ASAP
If you have any questions about tummy tucks, the friendly staff at our Vancouver clinic is available to assist you.
You are welcome to call us at (604) 874-2078 or you can book a consultation to speak directly with Dr. Gelfant.